

What Is Diabetes Melitus?
|
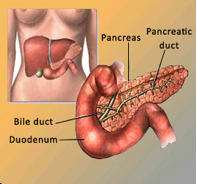
Diabetes Mellitus is a disorder which prevents the body from effectively utilising glucose. Simple carbohydrates (e.g. sugar in soft drinks or jam) and complex carbohydrates (rice or noodles) are broken down by the body to form glucose. The glucose in the bloodstream is subsequently metabolised by various tissues in the body and this process is regulated by insulin. Insulin is a hormone produced by the pancreas, a small organ located behind the stomach. Insulin deficiency and/or insulin resistance prevents glucose from entering cells to be used as a source of energy. This causes glucose to accumulate in the blood stream, resulting in diabetes mellitus.
|
 |
What Is Meant By Gestational Diabetes Mellitus (GDM)?
Diabetes that developed only in pregnancy, is called Gestational Diabetes Mellitus (GDM). This is a serious condition affecting pregnant women who were previously healthy but detected to have elevated blood glucose levels during pregnancy .
What Is The Different Between GDM and Type I or II Diabetes?
- Patient already has diabetes before they get pregnant
Diabetes can be divided into Type 1 Diabetes Mellitus or Type 2 Diabetes Mellitus. Previously, Type 1 Diabetes was termed “Insulin Dependent Diabetes Mellitus” (IDDM) and Type 2 Diabetes was termed “Non-Insulin Dependent Diabetes Mellitus” (NIDDM). Over 90% of diabetes patients suffer from Type 2 Diabetes. For Type 1 Diabetes patients, the beta cells in the pancreas produce very litte insulin or none at all. For Type 2 Diabetes patients, the main pathology is insensitivity of the insulin receptors (or insulin resistance) and these patients are usually over-weight or obese. - GDM
During pregnancy, the various hormones produced by the placenta interferes with the action of insulin, causing insulin resistance. Hormones such as oestrogen, cortisol and human placental lactogen, disrupts insulin action. As the placenta continues to grow during the second and third trimester, more of these hormones are produced, resulting in an increase in insulin resistance. The pancreas responds by producing even more insulin to overcome the resistance. Failure to compensate results in GDM. The patient will usually recover following childbirth, however she remains at high risk of developing diabetes later on in life.
 |
 |
How Common Is GDM?
GDM is usually detected after the 24th week of pregnancy, and occurs in about 1-14% of pregnancies each year. If left undetected and untreated, GDM can cause many serious complications for the pregnant women and the fetus/baby.
Who Is At Risk Of Getting GDM?
DM can happen to anyone during pregnancy. However, there are certain risk factors associated with getting GDM, which includes:
| Family history of diabetes |
|---|
| – Women age > 25 years |
| – Being overweight or obese prior to pregnancy |
| – History of previous GDM |
| – Current obstetric problems (e.g. hypertension in pregnancy, polyhydramnios) |
| – History of big baby (> 4 kg), still birth or birth deformities |
| – Recurrent vaginal candidiasis or fungal skin infection |
SIGNS AND SYMPTOMS
Typically women with GDM have no signs or symptoms, although some women may suffer from excessive thirst, urinary frequency and lethargy. Most women with GDM do not have any risk factors. Your doctor should conduct the Modified Oral Glucose Tolerance Test (MOGTT) to detect GDM during your first antenatal visit if you have any risk factors, or in between week 24th and 28th of your pregnancy if you are at low risk. However, if your risk is high and the first test performed early during the pregnancy is negative then a second test is usually performed between 24th and 28th weeks of your pregnancy.
What Is An MOGTT?
This is a test conducted after the patient has fasted overnight, typically starting at 10 p.m. the night before. A blood sample will be taken in the morning. The patient is then required to drink a sugary drink (75 gm of glucose diluted in 250 ml of water), and another blood sample will be taken 2 hours later.
Results Interpretation
| Venous plasma glucose (mmol/l | ||
|---|---|---|
|
Fasting
|
2 hours post glucose load
|
|
| Normal |
< 5.1
|
< 7.8
|
| GDM |
>= 5.1
|
>= 7.8
|
TREATMENT
Treatment for GDM includes taking appropriate and adequate steps to ensure that your blood glucose levels are always within normal limits during the pregnancy. Your doctor will advise you to follow a suitable meal plan and to increase your level of physical activity to control your blood glucose level. You will also have to regularly monitor your blood glucose (ideally 4 to 6 times a day) to ensure that your blood glucose is well controlled. Some women with GDM will require insulin injections, in addition to practicing a healthy diet and being physically active, to achieve the desired glycaemic targets.
Oral anti-diabetic (OAD) medications are generally not recommended during pregnancy. However, several current research have shown that some OADs are safe for use during pregnancy. Your doctor may prescribe you an OAD if your blood glucose levels are not that high.
The good news is that regular blood glucose monitoring in addition to practicing a healthy diet and being physically active is enough to control your GDM whilst reducing the risk of adverse events for you and your baby.
After you have delivered your baby and the placental hormone no longer circulates in the body, your blood glucose levels will return back to normal (except if you already have diabetes before being pregnant, but was not diagnosed earlier). Therefore, you don’t have to be overly concerned about your condition. However, you still need to take good care of yourself and enjoy the pregnancy.
If you already have diabetes and plan to become pregnant, you have to work hard to control your blood glucose levels several months before conception, because research has shown that a high blood glucose during the first trimester increases the risk of congenital abnormalities.You are advised to attend a ‘pre-pregnancy care’ clinic before you try to get pregnant to ensure that your blood sugar control is excellent.
Why Is A Specific Diet Recommended?
A balanced and nutritious diet is essential to maintain good health in the pregnant women and a successful pregnancy. For women with GDM, a good diet will ensure that the blood glucose levels remain normal and generally this is the first step taken before initiating insulin injections. Attention should be given to total daily calorie intake and the choice of food consumed to ensure glycaemic control. The daily calorie requirement will increase by 300 calories during the second and third trimester. For example, if the total daily calorie requirement is 1,800 kcal normally (not pregnant) and the body weight remains stable, the total daily calorie requirement of 2,100 kcal will be required from 14 weeks gestation onwards till delivery.
Below are some suggestions for healthy eating that will help will glycaemic control:
- Avoid sweets and food with high sugar content (e.g. cakes, ice creams, junk foods, soft drinks, canned fruits, jams, chocolates)
- Take complex carbohydrates (e.g. cereals, nuts, peas, vegetables and starchy food)
- Take high fibre food (e.g. fruits, vegetables, legumes, wholemeal breads)
- Ensure a low fat diet, especially saturated fats (butter, fatty meat, cream). Choose thin slices of beef or skinless chicken
- Avoid oily and deep fried food
Do You Have To Exercise?
Frequent physical activity of moderate intensity can reduce the risk caused by GDM by increasing insulin sensitivity in the cells, resulting in better glycaemic control. It also helps in preventing other discomforts associated with pregnancy such as constipation, back ache and muscle cramps.
Walking, stretching and light weight lifting will help you sweat during pregnany. Start with 15 minute sessions three times a week, then slowly increase the frequency and duration of exercise at your own pace and comfort. Take plenty of fluids to prevent dehydration and be alert when exercising during pregnancy. The extra weight in your abdomen will shift your centre of gravity, increasing your risk of falling. Therefore, avoid any activity which results in body instability. Stop exercising if you suffer from any headaches, dizziness, shortness of breath, feeling light-headed, palpitations, back pain, pelvic pain or vaginal bleeding. 3
What Happens If Diet Control And Exercise Fails To Control The Blood Glucose Levels?
In some cases, although you are already strictly controlling your diet and performing regular exercise, your blood glucose levels remain elevated. In this situation, your doctor may prescribe insulin injections. Insulin cannot be taken orally since it will be destroyed by gastric juices. Insulin is safe to use during pregnancy and is only a temporary measure since your blood glucose will return back to normal after delivery.
Insulin is given via an injection just under the skin using a very fine needle, resulting in just minor discomfort during the injection. It can be self-administered and you will be taught by your doctor or nurse on the injection techniques. The amount of insulin required to maintain glycaemic control will increase as the pregnancy progresses. This does not mean that your GDM is getting worse. The increase in the size of your placenta as pregnancy progresses results in increasing amount of hormones which counters the effects of insulin. Therefore, more insulin is required to overcome the effects.
How Do You Inject Insulin?
Your doctor or trained nurse will teach you the right insulin injection technique. It is a subcutaneous injection usually administered at the abdomen or thighs.

Insulin And Needle Care
Insulin must be kept in the dry area inside the refridgerator (e.g. the dairy produce section). You are encouraged to use a new needle for each injection. Repeated use of the same needle will cause it to become blunt, causing pain during injection.
Regular Blood Glucose Monitoring

Regular blood glucose monitoring is essential because the results indicate whether or not you are responding to treatment. It also helps you to determine if you require any changes in your dietary and physical activity program, and the doses of your medications. Ideally, you should check your blood glucose levels 4-7 times a day. You should take a fasting blood sample together with a one- or two-hour post-meal blood sample. Blood glucose measurements pre-meal and post-meal are encouraged since the results will help you adjust the amount of insulin required. There is also scientific evidence that controlling post-meal glucose levels results in better outcome for mother and baby as compared to controlling fasting blood glucose levels only. Your doctor may also advise you to check your blood glucose levels before and after exercising to avoid a hypoglycaemic attack during exercise.
During pregnancy, the recommended glycaemic targets will be tighter compared to a diabetes patient who is not pregnant. This is very important since abnormal blood glucose levels are associated with higher rates of complications for the pregnant mother and the fetus/baby. To reduce the risk for women with GDM, the recommended glucose level is ? 5.3 mmol/L (fasting and premeal) or ? 6.7 mmol/L (post-meal). Your doctor should discuss with you about your recommended targets for glycaemic control. Checking for glucose in the urine is not recommended as it is inaccurate particularly during pregnancy.
Alcohol Abstinence And Smoking Cessation
You are advised not to take alcohol throughout your pregnancy as this might adversely affect your pregnancy. Smoking cessation is also important as research has shown that exposure to cigarette smoke, even as a passive smoker, have a negative effect on the fetal development.
What Happens If You Experience Hypoglycaemia?
Low blood glucose (or hypoglycaemia) is a complication only associated with an individual on insulin injection. It may occur if you delay your breakfast or exercise more intensely than usual. It is a medical emergency and requires immediate intervention. If you experience any hypoglycaemic symptoms (e.g. confusion, dizziness, blurring of vision, sweating, tremors, extreme hunger), you have to immediately consume any form of sugar. When you are using insulin, you will have to bring along some sweets or food/drinks (e.g. sweet candy, glucose drinks) as a precautionary measure. Tell your doctor about any hypoglycaemic attacks that you may have experienced. Your doctor may want to change the dose or type of insulin used.
COMPLICATIONS
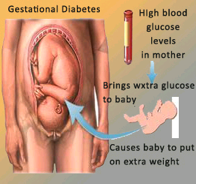
The rates of complications depends on your level of self-care. If your blood glucose levels are well controlled throughout your pregnancy, you can prevent the complications. If your blood glucose levels are high, it will be transferred to the fetus via the placenta, exposing the fetus to high levels of blood glucose. This will cause the fetal pancrease to react by producing more insulin to lower the blood glucose level. In addition, the fetus will also get excess energy (in the form of glucose) more than is required, and the excess energy will be stored as fat, resulting in macrosomia (defined as a baby born with body weight ? 4.0 kg).
The rates of complications depends on your level of self-care. If your blood glucose levels are well controlled throughout your pregnancy, you can prevent the complications. 8 If your blood glucose levels are high, it will be transferred to the fetus via the placenta, exposing the fetus to high levels of blood glucose. This will cause the fetal pancrease to react by producing more insulin to lower the blood glucose level. In addition, the fetus will also get excess energy (in the form of glucose) more than is required, and the excess energy will be stored as fat, resulting in macrosomia (defined as a baby born with body weight ? 4.0 kg).
The baby’s blood glucose levels will be closely monitored following delivery, and he/she may require intravenous glucose if the blood level is too low. The baby is also at risk of prolonged jaundice, electrolyte imbalances (e.g. low calcium and magnesium levels), breathing difficulties and congenital abnormalities. Macrosomic babies tend to develop into obese adults in the future, with the attendant increased risk of developing Type 2 Diabetes.
Ultrasound examination antenatally is useful to monitor the size of the growing fetus and to detect the presence of polyhydramnios. Like other diabetes patients, women with GDM is at high risk of experiencing complications such as urinary tract infections, diabetic ketoacidosis, and fungal skin infection. They are also susceptable for pre-term deliveries due to polyhydramnios and big baby.
GDM also causes complications during delivery, resulting in a difficult delivery and higher rates of Caesarean sections. You are also at higher risk of getting pre-eclampsia (high blood pressure which may be life-threatening) during the pregnancy. You are also at higher risk of getting GDM in future subsequent pregnancies. According to the National Institute of Health, USA, women with GDM has a 20-50% risk of getting Type 2 Diabetes in 5-10 years after delivery. This however, can be prevented – as shown in various landmark studies which demonstrated that lifestyle modification with or without pharmacological interventions for individuals at high risk (including women with GDM), reduced the risk of developing diabetes by 2-58%.
Will GDM Affect The Delivery Process?
GDM by itself is not an indication for a Caesarean section. However, if the baby is too big for a normal vaginal delivery, or if the baby cannot be delivered normally, a Caesarean section is then required. If the baby is too big, there is a risk of experiencing trauma during delivery, particularly bone fractures and nerve injuries at the shoulder region.
Keep Your Doctor’s Appointments
This is very important as your doctor will be able to detect early any complications for both the mother and the fetus, and intervene early before the condition worsens. When you are diagnosed with GDM, you may be advised to come for regular antenatal check-ups every two weeks until 32 weeks gestation, thereafter weekly visits to the clinic. During the visits, ultrasound examinations will be conducted to detect any congenital abnormalities, other complications, and monitoring the growth fo the fetus. Blood glucose monitoring will be conducted at least every two weeks to assess the effectiveness of treatment.
Close to delivery, you will be advised to monitor closely fetal movement, by for example, counting the number of ‘kicks’ that you experience.
There is a high possibility that your doctor will set a delivery date between the 38th to the 40th week of gestation because for women with GDM, the risk of complications increases after the 38th week If you require insulin therapy, you will be given an insulin injection in the morning before delivery, or the insulin may be given intravenously throughout the delivery process. After your baby is born, the blood glucose levels will return to normal and insulin will no longer be required.
An OGTT test is recommended 6-12 weeks post-delivery to ensure that the glucose levels have returned to normal. Following this, screening for Type 2 Diabetes should be done annually.
The good news is that although GDM can be a serious and dangerous condition, you can see that a well controlled diet together with regular exercise can help control your blood glucose levels and reduce the risk of complications for you and your baby. By following all of the guidelines above, you have a very good chance to deliver normally, giving birth to a healthy baby, even with GDM. More importantly, always discuss with the team managing your pregnancy how best to achieve all of the treatment targets.
Reference
1. Malaysian CPG on Management of Diabetes in Pregnancy
| Last Reviewed | : | 23 August 2019 |
| Writer | : | Dr. Mastura Ismail |
| Accreditor | : | Dr. Zanariah Hussein |
| Reviewer | : | Dr. Rafaie bin Amin |





