

Pleuroscopy or medical thoracoscopy is a minimally invasive procedure that allows access to the pleural space using a combination of viewing and working instruments.
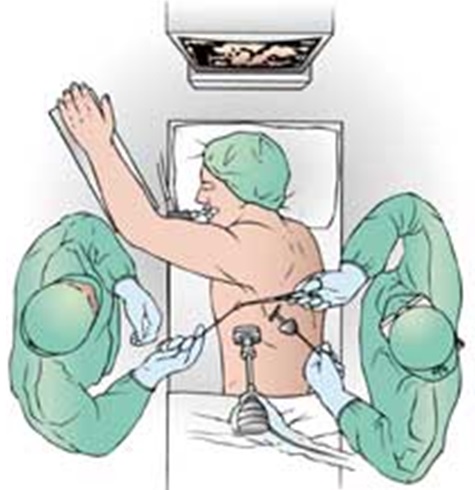
Sterile equipment for visualization, exposure, manipulation, and biopsy is required. A high-resolution video imaging system, which includes the pleuroscope (Figure 1), that allows all members of the team to view and participate in the procedure is beneficial to facilitate maximum assistance to the dedicated operator and safety for the patient (Figure 2). The procedure can be either performed in the operating room or in a dedicated environment for invasive procedures.
 |
| Figure 1 : A pleuroscope set |
 |
|
Figure 2. Patient, operator and video-imaging system |
Indications
- Diagnosis of unexplained collection of fluid in the pleural cavity
- Therapeutic procedure such as pleurodesis (a medical procedure in which the pleural space is artificially obliterated. It involves the adhesion of the two pleurae)
Contraindications
- Lack of a pleural space
- Uncorrected coagulopathy
- Hemodynamic instability
Patient Preparation
This procedure may be performed under local anesthesia with or without conscious sedation or under general anesthesia (patient is unconscious/asleep)
Pre-Procedure:
- A consent from the patient is required
- Blood investigations are done to ensure:
- Adequate blood levels
- No bleeding tendencies
- Other investigations such as:
- An electrocardiography (ECG)
- Lung functionare done for certain patients
- Patient is asked to fast overnight
- A cannula is inserted into the patient’s hand for injection of medication for sedation or fluids
During the Procedure:
- The patient is positioned in a lateral position with the side of affected area facing upwards
- The patient is padded comfortably, and secured to the table
- The site for pleuroscope entry into the pleural space is determined
- Standard sterile skin preparation and draping to create an adequate field are performed
- The skin is anesthetized with local infiltration anesthesia
- After ensuring adequate sedation, the pleural space is entered bluntly with a clamp passed over the rib and through the pleura (see chest tube insertion technique)
- With an adequate access space created, the pleural space immediately subjacent to the entry site is digitally inspected to ensure an adequate pleural space (freedom from pleural adhesions) to safely insert the pleuroscope
- The pleuroscope is inserted under direct vision into the pleural space (Figure 3)
- Once the surveillance panoramic examination is completed, the specific purpose of the procedure (eg, evacuation of pleural fluid, pleural biopsy, or pleurodesis) is addressed
- Fluid is evacuated using suction catheters passed through the working channel under direct vision
- Parietal pleural biopsy is performed with biopsy forceps passed through the working channel under direct vision
 |
|
Figure 3. The pleuroscope in the pleural space |
After the Procedure:
- Once the examination and procedure are completed, the pleuroscope is withdrawn
- A chest drain is placed, and the pneumothorax is evacuated
Complications
Complications of pleuroscopy are uncommon. These include:
- Bleeding
- Infection of the pleural space
- Injury to intrathoracic organs
- Collapse of the lungs
- Respiratory failure
References
- Chen LE, Langer JC, Dillon PA, et al. Management of late-stage parapneumonic empyema. J Pediatr Surg 2002; 37:371-374
- Danby CA, Adebonojo SA, Moritz DM. Video-assisted talc pleurodesis for malignant pleural effusions utilizing local anesthesia and IV sedation. Chest 1998; 113:739-742
- de Campos JR, Vargas FS, de Campos Werebe E, et al. Thoracoscopy talc poudrage: a 15-year experience. Chest 2001; 119:801-806
- Loddenkemper R, Schonfeld N. Medical thoracoscopy. Curr Opin Pulm Med 1998; 4:235-238
- Petrakis I, Katsamouris A, Drossitis I, et al. Video-assisted thoracoscopic surgery in the diagnosis and treatment of chest diseases. Surg Laparosc Endosc Percutan Tech 1999; 9:409-413
- Ronson RS, Miller JI Jr. Video-assisted thoracoscopy for pleural disease. Chest Surg Clin N Am 1998; 8:919-932
- Ross RT, Burnett CM. Talc pleurodesis: a new technique. Am Surg 2001; 67:467-468
- Seijo LM, Sterman DH. Interventional pulmonology. N Engl J Med 2001; 344:740-749
- Wilsher ML, Veale AG. Medical thoracoscopy in the diagnosis of unexplained pleural effusion. Respirology 1998; 3:77-80
| Last Reviewed | : | 13 November 2015 |
| Writer | : | Dr. Norhaya bt. Mohd Razali |
| Accreditor | : | Dr. Jamalul Azizi b. Abdul Rahaman |





